.jpg)
Ovarian cancer has long been called "The Silent Killer", because it usually isn't discovered until its advanced stages. In 70-75% of cases the cancer has spread to other parts of the abdomen before it is detected. However, the truth is that early-stage ovarian cancer often does produce symptoms – but they are subtle.
Just How Common Is Ovarian Cancer?
It is relatively rare, accounting for about 3 percent of all cases
of cancer in women. In general, your chances of getting ovarian cancer are 1 in
58 (compared to 1 in 7 for breast cancer), but the odds worsen as various risk
factors are considered.
Why Should I Worry About Ovarian Cancer?
You shouldn’t worry about it – but you should be aware of it and
take the steps to detect it at a stage when the chance of a cure is high. When
this cancer is found early and in still in the ovaries, there’s a 90 to 95
percent chance the patient will survive five years. When it is detected at an
advanced stage, the five-year survival rate drops to 18 percent.
At What Age Is Ovarian Cancer Most Likely to
Be Found?
It is most often found in women between the ages of 40 and 70 –
and women between 50 and 59 are in the high-risk group – but it sometimes
strikes women in their 20s. In fact, the Julie Merle Epstein Cancer Fund at
UConn Health was created to honor the memory of Julie, a woman who died from
ovarian cancer at the age of 28.
I Have a Pap Test Each Year. Will It Detect
Ovarian Cancer?
No. The Pap test detects cancer of the cervix, not cancer of the
ovaries.
What Should I Do to Detect Ovarian Cancer?
The best precaution is to have a complete pelvic exam done every
year by a physician who is aware of your family and medical history. It is
especially important for your doctor to be aware of any factors that place you
at high risk for this disease.
 The most important is a family history of ovarian cancer – a
mother, sister, or grandmother who had it. A history of breast or colorectal
cancer increases your risk, as does infertility or never having given birth to
a living child. The use of birth control pills or having several children is
associated with a lower risk for ovarian cancer.
The most important is a family history of ovarian cancer – a
mother, sister, or grandmother who had it. A history of breast or colorectal
cancer increases your risk, as does infertility or never having given birth to
a living child. The use of birth control pills or having several children is
associated with a lower risk for ovarian cancer.
The problem with ovarian cancer is that many of the symptoms are
easily confused with digestive disorders and bladder problems, so the cancer
goes unrecognized until it's advanced.
Many women with ovarian cancer realize they were experiencing unexplained symptoms for months, even years, before their cancer was diagnosed. Recently, researchers found that ovarian cancer could be detected using a blood test in combination with a simple screening. Women should check with their doctors if they notice one or more of these symptoms:
Many women with ovarian cancer realize they were experiencing unexplained symptoms for months, even years, before their cancer was diagnosed. Recently, researchers found that ovarian cancer could be detected using a blood test in combination with a simple screening. Women should check with their doctors if they notice one or more of these symptoms:
·
Pelvic or abdominal pain
·
Increased abdomen size or bloating
·
Feeling constantly full or having difficulty eating
Of course, these symptoms are common to many
conditions. But if the symptom is new, and persists over time, talk to your
doctor.
Other signs reported by ovarian cancer patients:
·
Abdominal cramping
·
An urgent need to urinate
·
Urinary burning or discharge
·
Indigestion or nausea that persists over a long period of time
·
Frequent episodes of gas
·
Unexplained constipation
·
Unexplained increase in waist size "“ i.e. you can't zip up
your jeans
·
Pain during sex
·
Lower back pain
·
Menstrual changes such as more pain during periods or heavier
bleeding
·
Lack of energy
Those with a family history of breast or
ovarian cancer should be even more vigilant; talk to your doctor about genetic
screening and be alert to any new symptoms in the pelvic area.
.jpg)
Services for Women at Higher Risk
Although researchers are trying to find ways to identify “tumor
markers” (substances in the blood or urine that may reveal cancer before
symptoms develop), there currently is no screening exam to detect this cancer
in women without symptoms.
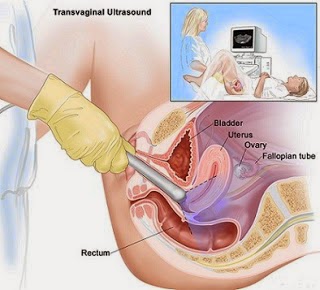
However, women at higher risk can take advantage of frequent
screening tests, including transvaginal ultrasound of the ovaries and in some
cases, blood tests.
If cancer is suspected, exploratory surgery may be done so the
doctor can see the ovaries and take tissue samples. If tests of the samples
reveal cancer, then appropriate surgery is the initial phase of treatment,
after which chemotherapy may be used.
Please
scan and email your medical reports to us at care@medworldindia.com and we
shall get you a Free Medical Opinion from India’s Best Doctors.
Call Us : +91-9811058159
Mail Us : care@medworldindia.com

.jpg)
.jpg)

.jpg)
.jpg)




